Anatomy of Volleyball
Since the sport requires a variety of movements, different bones, joints and muscles are stressed with each specific skill in volleyball. Here we will look at and break down the muscles and joints required to make a pass and take a look at arm swing and common injuries occurred from "spiking".
Before we get into the muscles involved in these skills, let's take a deeper look at what a muscle is and how it contracts...
Before we get into the muscles involved in these skills, let's take a deeper look at what a muscle is and how it contracts...
Muscle Tissue
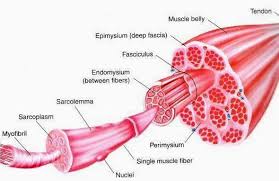
Muscles are made of bundles of cylindrical cells that are striated, known as fibres. So a muscle is composed of bundles of fascicles, which are made up of bundles of muscle cells, which is composed of myofibrils, and myofibrils are formed through bundles of myofilaments. The body is composed of 3 different muscle fibre types, and everyone has a different combination of these three types.
1. Slow Twitch Fibres (Type I): These fibres contract slowly, but repeatedly over long periods of time. The blood flow to these muscles is good and so these fibres are favoured for endurance activities using the aerobic energy system that relies on a supply of oxygen (will learn more about this under physiology). Commonly known as 'red fibres'.
2. Fast Twitch Fibres (Type IIA): fast twitch fibres have a quick contraction speed and either uses aerobic (oxygen dependant) sources of energy as well as anaerobic (no oxygen used) energy sources. These are known as 'white fibres' since they are not as reliant on oxygen supply from the blood and fatigue faster than slow twitch fibres. Used in activities such as fast running events like 400m and lifting moderately heavy weight for 8-12 repetitions.
3. Fast Twitch Fibres (Type IIB): These fibres contract very rapidly and creates forceful muscle contractions, fatiguing quickly. They are also 'white fibres', but strictly depend on anaerobic energy sources. Activities such as heavy weight lifting, sprinting short distances and explosive short movements.
MUSCLE CONTRACTION-SLIDING FILAMENT THEORY:
Step 1: Calcium ions flood the cytosol of the muscle cell, exposing the binding sites on actin.
Step 2: Myosin forms the cross bridge with actin
Step 3: “Power stroke” the myosin pulls the actin using ATP towards the centre of the sarcomere.
Step4: Troponin breaks the cross bridge formed between myosin and actin. ATP fuels this step.
Step 5: The hydrolysis of ADP+Pi which re-energizes the cross bridge. Steps 2-5 are repeated over, as contractions are needed in the muscle.
Step 6: The calcium ions are returned to the sarcoplasmic reticulum through active transportation. Binding sites on actin are covered again by Troponin and Tropomyosin.
1. Slow Twitch Fibres (Type I): These fibres contract slowly, but repeatedly over long periods of time. The blood flow to these muscles is good and so these fibres are favoured for endurance activities using the aerobic energy system that relies on a supply of oxygen (will learn more about this under physiology). Commonly known as 'red fibres'.
2. Fast Twitch Fibres (Type IIA): fast twitch fibres have a quick contraction speed and either uses aerobic (oxygen dependant) sources of energy as well as anaerobic (no oxygen used) energy sources. These are known as 'white fibres' since they are not as reliant on oxygen supply from the blood and fatigue faster than slow twitch fibres. Used in activities such as fast running events like 400m and lifting moderately heavy weight for 8-12 repetitions.
3. Fast Twitch Fibres (Type IIB): These fibres contract very rapidly and creates forceful muscle contractions, fatiguing quickly. They are also 'white fibres', but strictly depend on anaerobic energy sources. Activities such as heavy weight lifting, sprinting short distances and explosive short movements.
MUSCLE CONTRACTION-SLIDING FILAMENT THEORY:
Step 1: Calcium ions flood the cytosol of the muscle cell, exposing the binding sites on actin.
Step 2: Myosin forms the cross bridge with actin
Step 3: “Power stroke” the myosin pulls the actin using ATP towards the centre of the sarcomere.
Step4: Troponin breaks the cross bridge formed between myosin and actin. ATP fuels this step.
Step 5: The hydrolysis of ADP+Pi which re-energizes the cross bridge. Steps 2-5 are repeated over, as contractions are needed in the muscle.
Step 6: The calcium ions are returned to the sarcoplasmic reticulum through active transportation. Binding sites on actin are covered again by Troponin and Tropomyosin.
Forearm Passing "bump"
Lower Body Bones:
Femur
Fibula
Tibia
Tarsals, Metatarsals, Phalanges
Lumbar region
Sacrum
Lower Body Muscles:
Gluteal Group
Hamstrings
Quadriceps
Gastrocnemius
Tensor Fascia Latae
Rectus Femoris
Tibialis Anterior
Upper Body Bones:
Scapula
Thoracic and Cervical regions
Humerus
Ulna
Radius
Carpals, Metacarpals, Phalanges
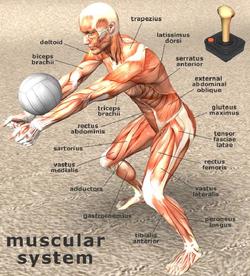
Upper Body Muscles:
Deltoids
Trapezius
Latissimus Dorsi
Rectus Abdominus
Joints used:
Hip Joint-a synovial ball-and-socket joint formed between the os coxa and the femur. The round, inner crest called the acetabulum forms the socket, and the round head of the femur creates the ball. This allows it to be one of the most flexible joints in the body, next to the shoulder. Major ligaments involved include the iliofemoral, pubofemoral, and ischiofemoral ligaments.
Knee Joint- Composed of the articulation of the femur and the tibia, and classified as a modified hinge joint. The knee also has the function of slight rotation medially or laterally that can also classify it to be a ellipsoid joint as well. The patella of the knee which is wrapped within a tendon is known as a sesamoid bone. Major ligaments include collateral, patellar, fibular, posterior cruciate (PCL), tibial, anterior cruciate (ACL) and medial collateral (MCL) and oblique popliteal ligaments. Major tendons include patellar, gastrocnemius , adductor magnus, semimembranosus, and popliteal tendons. Also, the meniscus both medial and lateral are worth mentioning as it is the cartilage that cushions the joint and is vulnerable to tears through rotation of the knee.
Ankle Joint- a modified hinge joint that is composed of the distal ends of the fibula and tibia resting on the talus. It allows for plantar flexion and dorsiflexion. The joint is wrapped with a thick fibrous capsule. The crucial ligaments in the ankle includes the anterior and posterior tibiofibular ligaments and the calcaneofibular ligament. These are also the weakest ligaments and are easily damaged when rapidly changing direction or jumping. A major tendon is the calcanea tendon, better known as the Achilles tendon.
Femur
Fibula
Tibia
Tarsals, Metatarsals, Phalanges
Lumbar region
Sacrum
Lower Body Muscles:
Gluteal Group
Hamstrings
Quadriceps
Gastrocnemius
Tensor Fascia Latae
Rectus Femoris
Tibialis Anterior
Upper Body Bones:
Scapula
Thoracic and Cervical regions
Humerus
Ulna
Radius
Carpals, Metacarpals, Phalanges
Upper Body Muscles:
Deltoids
Trapezius
Latissimus Dorsi
Rectus Abdominus
Joints used:
Hip Joint-a synovial ball-and-socket joint formed between the os coxa and the femur. The round, inner crest called the acetabulum forms the socket, and the round head of the femur creates the ball. This allows it to be one of the most flexible joints in the body, next to the shoulder. Major ligaments involved include the iliofemoral, pubofemoral, and ischiofemoral ligaments.
Knee Joint- Composed of the articulation of the femur and the tibia, and classified as a modified hinge joint. The knee also has the function of slight rotation medially or laterally that can also classify it to be a ellipsoid joint as well. The patella of the knee which is wrapped within a tendon is known as a sesamoid bone. Major ligaments include collateral, patellar, fibular, posterior cruciate (PCL), tibial, anterior cruciate (ACL) and medial collateral (MCL) and oblique popliteal ligaments. Major tendons include patellar, gastrocnemius , adductor magnus, semimembranosus, and popliteal tendons. Also, the meniscus both medial and lateral are worth mentioning as it is the cartilage that cushions the joint and is vulnerable to tears through rotation of the knee.
Ankle Joint- a modified hinge joint that is composed of the distal ends of the fibula and tibia resting on the talus. It allows for plantar flexion and dorsiflexion. The joint is wrapped with a thick fibrous capsule. The crucial ligaments in the ankle includes the anterior and posterior tibiofibular ligaments and the calcaneofibular ligament. These are also the weakest ligaments and are easily damaged when rapidly changing direction or jumping. A major tendon is the calcanea tendon, better known as the Achilles tendon.
Taking a look at the Joints-Slide Show
Volleyball Jump Attack
This offensive move requires a 3-5 step approach, a vertical jump and an arm swing. Because of the variety of movements, the change of direction and use of synovial joints, there is a lot of room for things to go wrong and injuries to happen. Let's first look at the lower body injuries, although mostly uncommon, they can happen with over use and freak accidents.
Potential injuries:
ankle sprain/fractures (primarily inversion)
patellar tendonitis (jumper's knee)
shin splints
strained hamstrings
These injuries can be detected and deciphered using the following tests:
Active Movement Test (Fracture)
Passive movement Test (Sprain)
Resisted Movement Test (Strain)
Potential injuries:
ankle sprain/fractures (primarily inversion)
patellar tendonitis (jumper's knee)
shin splints
strained hamstrings
These injuries can be detected and deciphered using the following tests:
Active Movement Test (Fracture)
- initiated by the athlete (contracts muscle)
- determine if pain increases
- look for irregular (trick) movements
Passive movement Test (Sprain)
- joint is moved through the range of motion by the trainer (athlete’s muscles not doing the work)
- determine if pain increases
Resisted Movement Test (Strain)
- Joint position does not change (no movement)
- Determine if pain increases
- Look for weakness
Shoulder Joint injuries
Shoulder injuries are the fourth most popular injury volleyball players face and can account for up to 20% of all injuries obtained in both men’s and women’s divisions. Although they fall behind ankle, knee and spinal injuries, they can still be equally as painful and severe, placing some athletes off the court for an entire season. With an estimated value of 40, 000 spikes for an athlete per season, volleyball players are most prone to overuse injuries. Majority of the injuries obtained are a result of overuse or muscular imbalance and can be avoided by taking precautionary measures. Common injuries volleyball players face include:
biceps tendinitis- caused by the overuse or lack of rest for the biceps brachii muscle. This injury causes pain in the anterior side of the shoulder which is the result of the inflammation of the biceps tendon within the intertubercular groove. Biceps tendinitis can be treated with rest, icing and non steroidal anti inflammatory drugs (NSAID’s).
rotator cuff tear- Since the supraspinatus, infraspinatus, subscapularis and teres minor have a common tendinous insertion located on the greater tubercle, if a part of the tendon is torn, all four muscles are affected, causing a great deal of pain based on the severity of the tear. The tendon can be torn through overuse and thus makes volleyball players more prone to the injury, with the frequency of arm swings required in the sport. Players with torn rotator cuffs face stiffness, limited range of motion and pain with movement, which can be dealt with through physical therapy and depending on severity, surgery. Therapy focuses on strengthening the surrounding muscles like the supraspinatus and steroid injections can serve as another option, helping with the inflammation surrounding the joint.
shoulder separations- tearing of the acromioclavicular ligament that holds the acromioclavicular joint (AC joint) together. This is very common in beach volleyball and in the libero position in indoors, with the repetitive diving motion while extending the shoulder overhead. The severity of separation is determined by the extent the clavicle has been separated from the acromion and is evaluated by degree. The higher the degree, the greater need for surgical repair and intensive rehabilitation.
biceps tendinitis- caused by the overuse or lack of rest for the biceps brachii muscle. This injury causes pain in the anterior side of the shoulder which is the result of the inflammation of the biceps tendon within the intertubercular groove. Biceps tendinitis can be treated with rest, icing and non steroidal anti inflammatory drugs (NSAID’s).
rotator cuff tear- Since the supraspinatus, infraspinatus, subscapularis and teres minor have a common tendinous insertion located on the greater tubercle, if a part of the tendon is torn, all four muscles are affected, causing a great deal of pain based on the severity of the tear. The tendon can be torn through overuse and thus makes volleyball players more prone to the injury, with the frequency of arm swings required in the sport. Players with torn rotator cuffs face stiffness, limited range of motion and pain with movement, which can be dealt with through physical therapy and depending on severity, surgery. Therapy focuses on strengthening the surrounding muscles like the supraspinatus and steroid injections can serve as another option, helping with the inflammation surrounding the joint.
shoulder separations- tearing of the acromioclavicular ligament that holds the acromioclavicular joint (AC joint) together. This is very common in beach volleyball and in the libero position in indoors, with the repetitive diving motion while extending the shoulder overhead. The severity of separation is determined by the extent the clavicle has been separated from the acromion and is evaluated by degree. The higher the degree, the greater need for surgical repair and intensive rehabilitation.
